Science reporting frequently fails to meaningfully communicate research results, especially when it comes to medical research. Out of context numbers and percentages only create public misunderstanding of the scientific results.
When the LA Times published Karen Kaplan’s comparison of the Moderna and Pfizer COVID-19 vaccines consisting essentially of a list of percentages without explanation, it created the impression that one vaccine was better than the other for certain populations. Asian parents sent the article to their children urging them to get the Moderna vaccine if possible. Yet these numbers were calculated with a sample size too low to make even a guess of that conclusion.
Many people have seen in numerous news stories and press releases that both of these vaccines have about 95% efficacy. But news stories don’t explain how these numbers are calculated. Vaccine efficacy (VE) is calculated by comparing the difference in rate of infection between the vaccinated group and the placebo group.
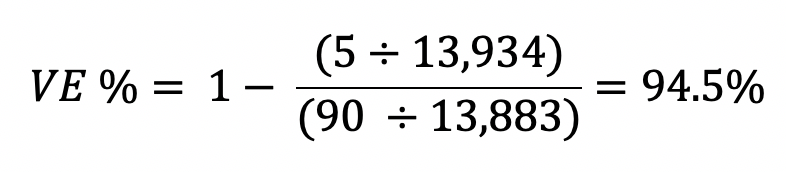
The efficacy calculation used in these vaccine trials is reduction in relative risk in the vaccinated group, calculated with this formula:

In the Moderna vaccine trial, 13,934 study participants received the vaccine and five of those participants developed COVID-19. 13, 883 participants received the placebo and 90 of those participants developed COVID-19. (Source: Page 23, Table 9 of FDA Moderna briefing document)
In the Pfizer vaccine trial, 18,198 study participants received the vaccine and eight of those participants developed COVID-19. 18,325 participants received the placebo and 162 of those participants developed COVID-19. (Source: Page 24, Table 6 of FDA Pfizer briefing document)

These numbers answer the question the LA Times poses, “how effective are the vaccines overall?” The FDA had signaled it was prepared to consider emergency use authorization to any vaccine with over 50% efficacy and these VE percentages were well above that threshold.
But then, the LA Times article goes on to ask the same question for different populations and answers it based on the VE % for different subgroups published in the study data. The problem is that many of these subgroups do not have a large enough sample size of study participants who developed COVID-19 for this VE % to be statistically evaluable.
The data are displayed in the documents for completeness, but any difference between the subgroup VE % and the overall VE % is most likely due to chance. Publishing these numbers as if the Pfizer vaccine is 100% effective in Pacific Islanders when there was only one case of COVID-19 among Pasifika participants for the analysis is irresponsible and misleading.
Calculations for how each VE % published in the LA Times article are shown in the following table and shows how absurd it is to conclude that one vaccine is better than the other for any of these subgroups. The comparisons made were not always even between subgroups of the same criteria, showing the VE % for ages 65+ for the Moderna trial and ages 56+ for the Pfizer trial in the evaluation of whether these vaccines are effective in older people.
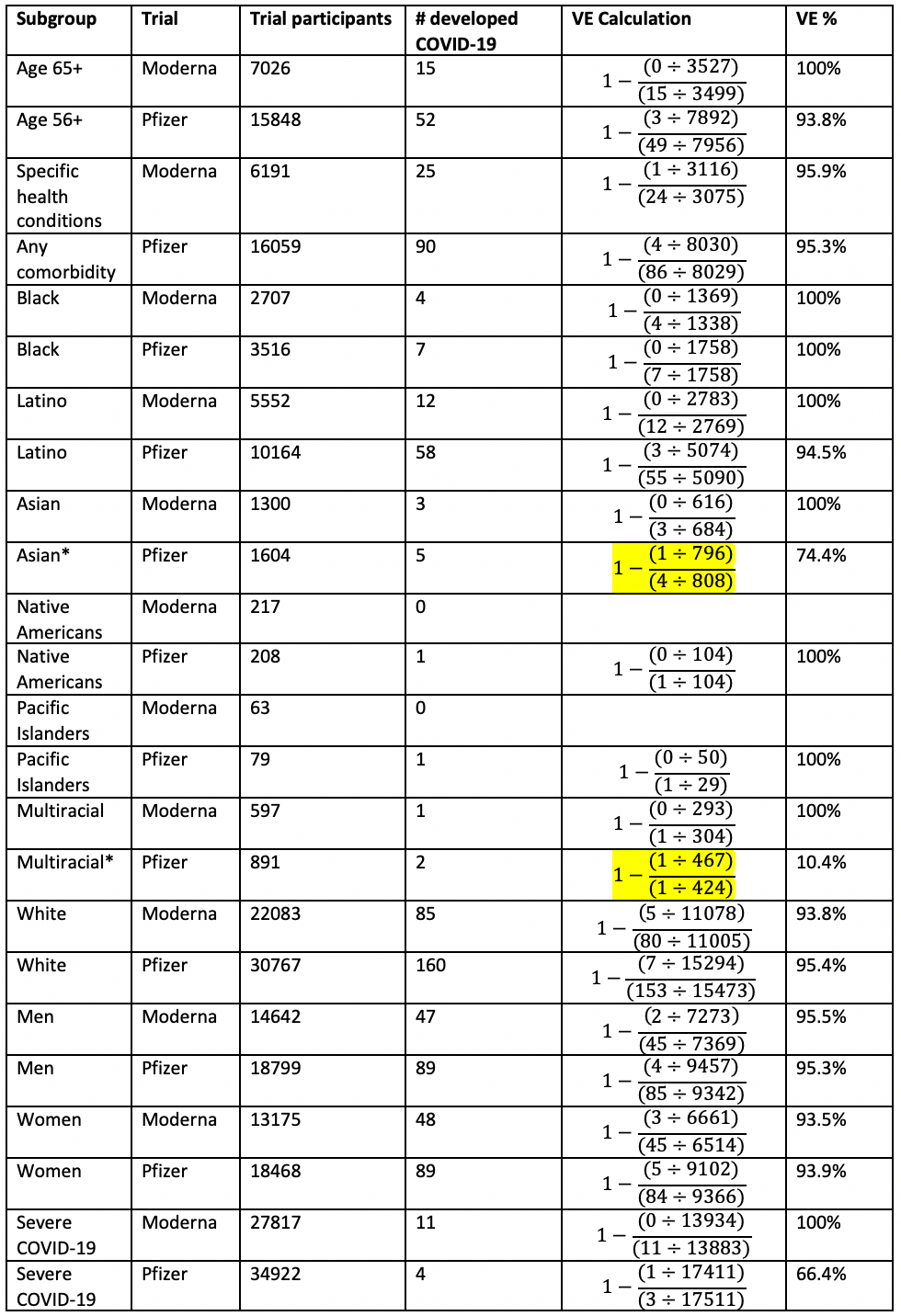
There simply is not enough data to assess efficacy among groups that make up a small percentage of the trial participants. While there are efforts to recruit people of color and older trial participants and most of these trials end enrollment for younger white people once they reach certain overall enrollment goals, it would take thousands more Asian, Black, and other trial participants to make any meaningful assessment on the vaccine’s efficacy for any of these specific groups.
Likewise, the reporting on the MIT machine learning study, such as this Yahoo report wrongly implies that the Pfizer and Moderna vaccines may not be as effective for Asian and Black participants:
“Researchers used artificial intelligence and machine learning to examine a vaccine similar to these big developers', and found that while less than 0.5 percent of white trial participants didn't respond strongly to the vaccine, nearly 10 percent of Asian participants didn't.”
This is misleading and overblows the potential racial disparity in vaccine efficacy. For a summary of the immunological reasons for this, please refer to this Twitter thread by professor of immunology Akiko Wasaki. Yahoo also reports on the study as if it were a clinical trial performed on real people, but it was a computer simulation that modeled theoretical vaccines.
The MIT study found striking simulated racial disparities for a predicted vaccine that only encodes the receptor binding domain (RBD) of the spike protein. 37.3% of Asian people's immune systems wouldn't be able to recognize an RBD vaccine.
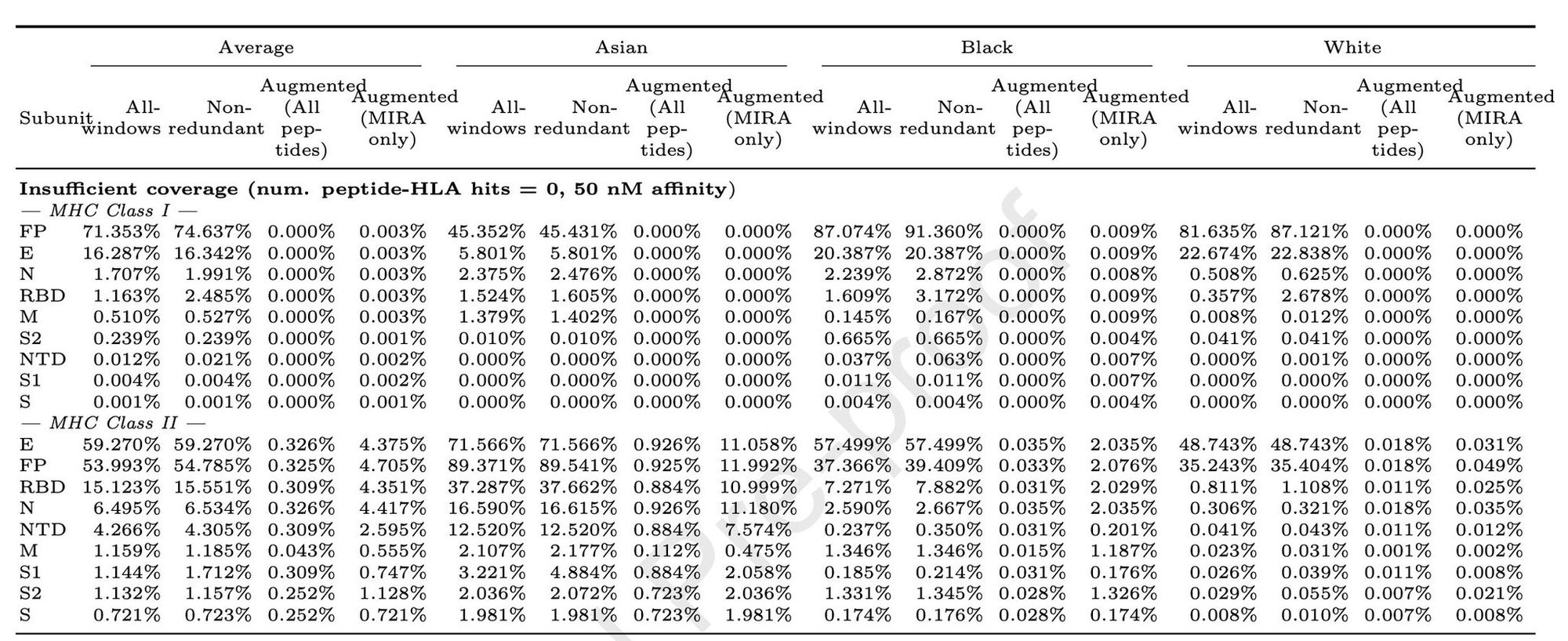
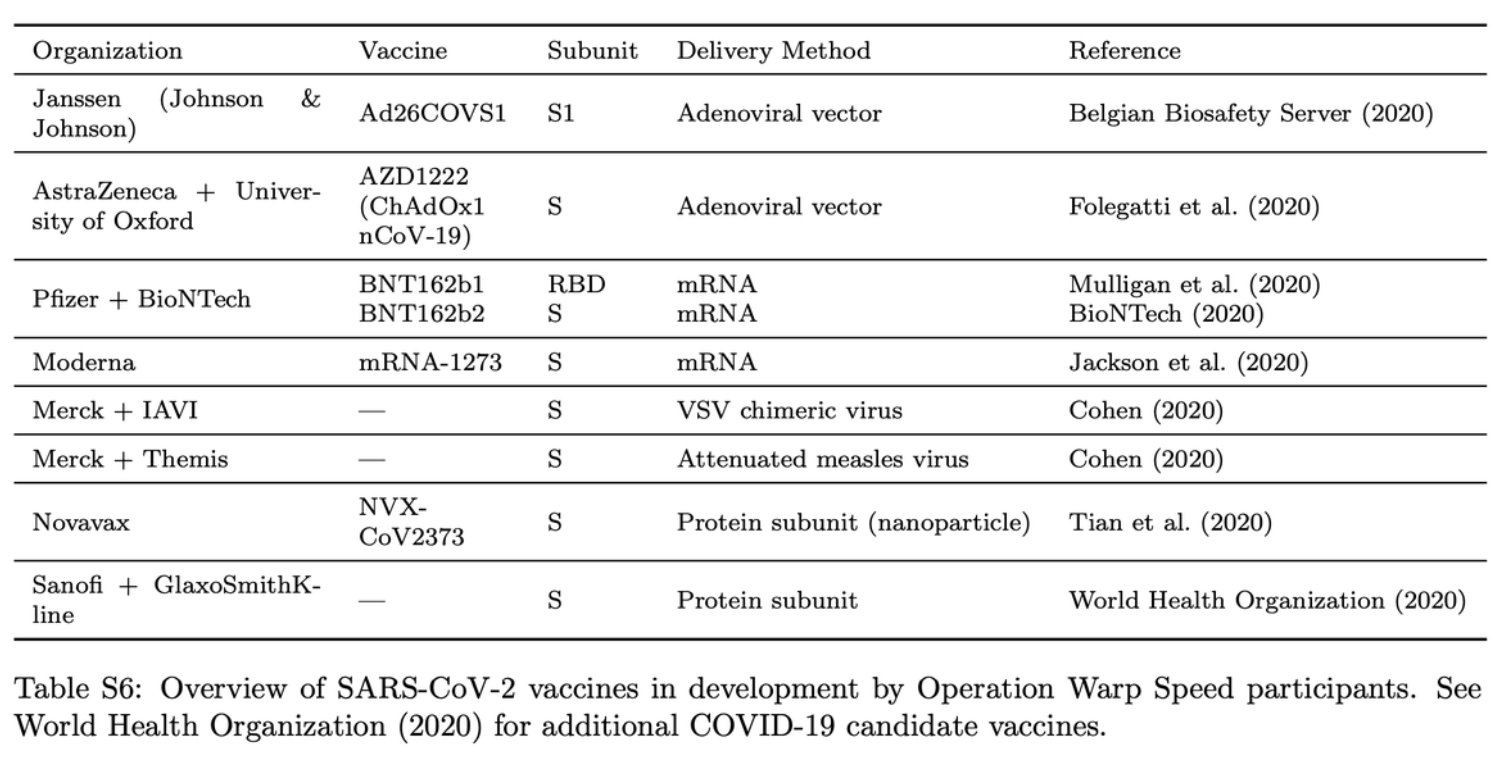
However, Moderna's vaccine encodes the entire spike protein. Astrazeneca's vaccine encodes the entire spike protein. Pfizer performed trials on two vaccine variants: one encoding only the RBD and one with whole spike protein. The whole spike protein version of Pfizer's vaccine is the only one approved for emergency use in the UK and US. The MIT study actually predicts more than 98% robust coverage for every demographic group for a vaccine that encodes the whole spike protein.
The study does say that vaccines which contain the whole virus, or at least includes more than one viral protein, are more robustly effective than a vaccine which only expresses the spike protein. For example, we can infer from the MIT study that SinoVac’s inactivated virus vaccine is more effective than any vaccines developed by Operation Warp Speed. However, the MIT study suggests that all the vaccines developed by these US companies are predicted to be effective for most people in every demographic group as well.
Additionally, Asian, Black, and other people of color continue to be specifically recruited for trials in order to have diversity in participants. Many trials are beginning to exclusively recruit older people (also underrepresented in trials but overrepresented in COVID infections and deaths) or people of color to prove their efficacy across more demographic groups.
There are two take-home messages we’d like to focus on.
1. Much of the scientific journalism on America’s COVID vaccines has been inaccurate, misleading, fearmongering, and irresponsible. That should make people think extra hard about how poorly represented the Chinese (and likely future other non-Western) vaccines are in any reporting on them done by Western corporate media.
2. The US clearly has enough problems to worry about with domestic COVID containment, vaccine production and distribution, and lack of clear and accurate reporting of information to the people. American corporate media should stop wasting its time speculating on China’s vaccines and COVID caseload from last winter. These are racist distractions that only hurt Americans further.

Comments powered by Talkyard.